
Understanding the Types of Spinal Fractures: A Guide to Back Injuries
Updated:
When we think of a broken bone, most of us imagine a cast and a few weeks of recovery. But spinal fractures are much more complex. Your spine, made up of 33 vertebrae, is not just a structural pillar—it also protects the spinal cord. A fracture in this area can affect mobility, cause severe pain, and even threaten neurological function. In this post, we’ll explore the main types of spinal fractures, what causes them, and how they’re treated.
What Is a Spinal Fracture?
A spinal fracture occurs when one or more of the vertebrae in the spine break or collapse. These injuries range from minor compression fractures to more serious burst or fracture-dislocation types, potentially damaging the spinal cord.
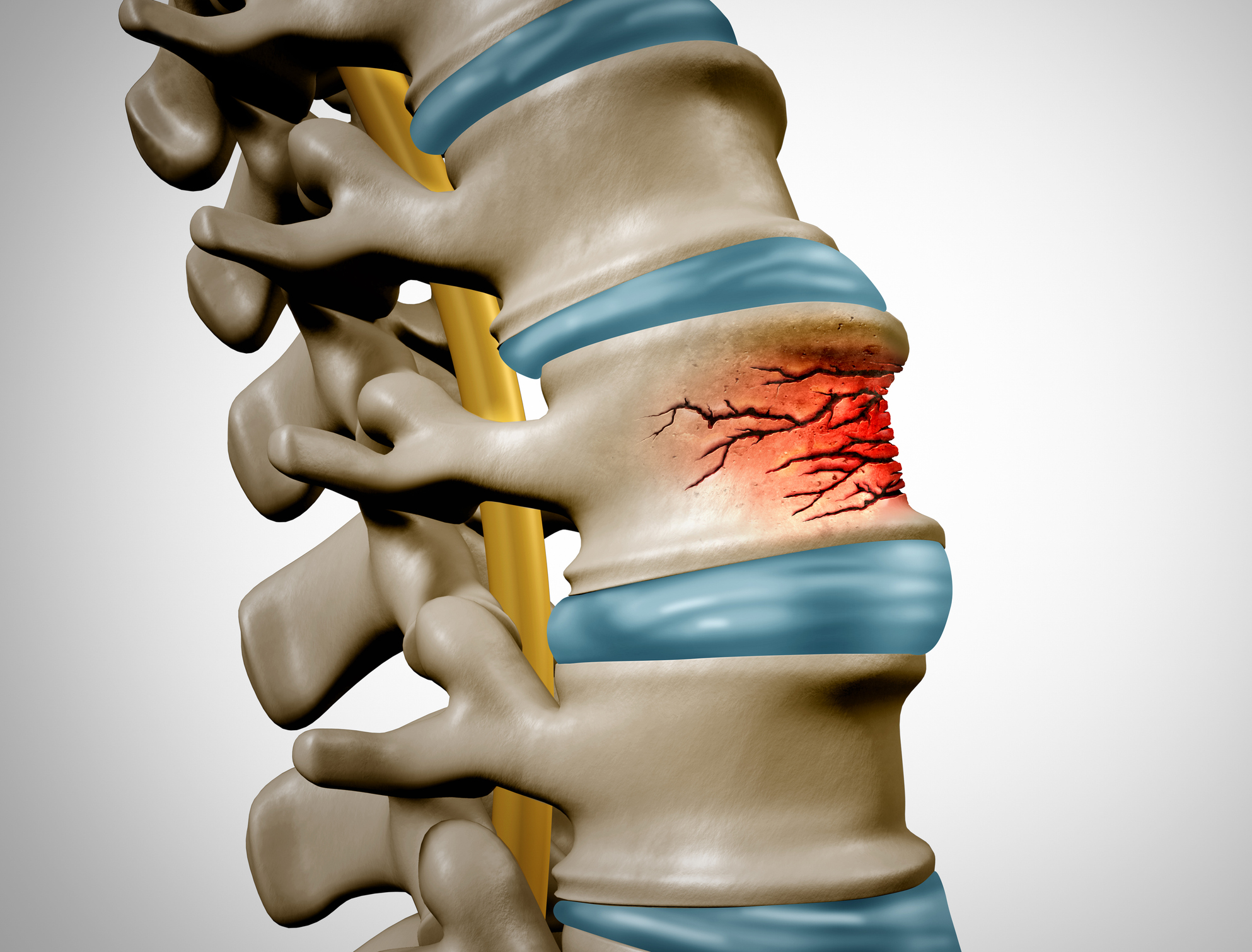
1. Compression Fracture
What it is:
A compression fracture happens when the front part of a vertebra collapses, while the back remains intact. This wedge-shaped deformation often results from osteoporosis, especially in older adults.

Common symptoms:
- Sudden back pain from a trivial fall or lifting strain
- Loss of height over time
- Hunched posture (kyphosis)
Treatment:
Usually nonsurgical—pain management, rest, and very rarely spinal bracing. Usually heal naturally within 6-12 weeks. Diagnosis can usually be made with a simple X-ray.
However – If the pain is severe and/ or associated with an obvious loss of height or progressive stoop seek specialist help immediately to get the best long-term result and get yourself out of pain. Untreated osteoporotic fractures with persistent symptoms are a huge cause of pain and disability in the community.
Severe cases like this require prompt intervention with procedures like vertebroplasty or balloon kyphoplasty.
2. Burst Fracture
What it is:
This occurs when a vertebra is crushed with a violent axial compression force, typically due to a high-impact trauma like a car accident or a fall from a significant height.
These are commonly in the thoracic or lumbar spine. Lumbar spine injuries carry a better prognosis.
These can be stable (able to withstand physiological load) or unstable leading to deformity or neurological damage under load (standing).
Common symptoms:
- Severe back pain, sometimes inability to move or roll over due to pain.
- Numbness or weakness in the legs – a bad sign, see below
- Risk of spinal cord injury causing paraplegia
Treatment:
Often surgical, involving reconstruction, spinal fusion and stabilization to prevent further damage and correct deformities. Particularly for unstable fractures.
Stable fractures can be treated non operatively with bedrest, analgesia and then mobilisation. A spinal brace can be used depending on the fracture, and regular follow up X-rays should be taken.
The reassuring news is that the prognosis with either form of treatment is good.
3. Flexion-Distraction Fracture
What it is:
This injury usually occurs in car accidents when the upper body is thrown forward while the pelvis is held in place by a seatbelt. It causes the vertebra to pull apart. As it sounds, these are some of the worst injuries, are usually unstable, and can be life threatening.
Common symptoms:
- Severe and immediate unremitting pain
- Possible abdominal injuries (due to seatbelt pressure) causing shock and abdominal pain. This can be worse than the back pain in the first instance.
Treatment:
Surgical stabilization is often necessary, sometimes as an emergency, especially if there’s ligament damage, spinal instability or neurological deficit.
4. Fracture-Dislocation
What it is:
This is a severe injury where a vertebra both fractures and moves out of alignment with the adjacent vertebrae. It almost always causes spinal instability and often affects the spinal cord. This is very rare in the thoracic or lumbar spine but more common in the cervical spine. It can be caused in sports such as rugby ( a collapsed scrum) martial arts, or high energy vehicle trauma.
Common symptoms:
- Intense pain and inability to move or stand
- Shooting Leg pain or arm pain
- Acute and immediate neurological deficits (like paralysis or loss of bladder control)
Treatment:
Emergency surgery is typically required to realign and stabilise the spine but also relieve any pressure on the spinal cord.
Risk Factors and Prevention
Who is at risk?
- Older adults (especially those with osteoporosis)
- Athletes in high-impact sports
- High risk sports such as motor racing, parachuting, paragliding, climbing
- Motor cyclists
- Off Road Mountain biking
- Victims of high-velocity accidents
- People working at height (Windfarm engineers, roofers)
- Individuals with certain cancers (that weaken the bones)
Prevention tips:
- Maintain strong bones with calcium and vitamin D
- Treat any underlying osteoporosis
- Regular weight-bearing exercise
- Fall-proof your home if you’re more elderly and at risk
- Use seatbelts and safety gear – Don’t forget to clip on!

When to See a Spine Consultant
Any injury involving the back—especially with severe pain, weakness, or numbness—should be evaluated by a spinal consultant or trauma surgeon as an emergency. Early intervention can prevent long-term complications and improve outcomes. This is normally done in the NHS as part of trauma management for the more acute, severe injuries.
Final Thoughts
Osteoporotic compression fractures are not one-size-fits-all. Seeking specialist assessment early if things aren’t going well is crucial to effective treatment and recovery. Getting the right help can make all the difference.
Contact the Experts at SpineArt
At SpineArt, we specialise in diagnosing and treating osteoporotic fractures and sportsmen with low energy injuries. We use personalised, evidence-based care. Our spinal consultant, Mr. Dan Fagan, has extensive experience in managing these conditions.
Mr. Fagan offers private consultations at the following locations:
- Nuffield Health Tees Hospital, Stockton
- Woodlands Hospital, Darlington
Telemedicine consultations are also available online.
Get in touch today to book a consultation with Mr. Dan Fagan at SpineArt.







